Symptoms
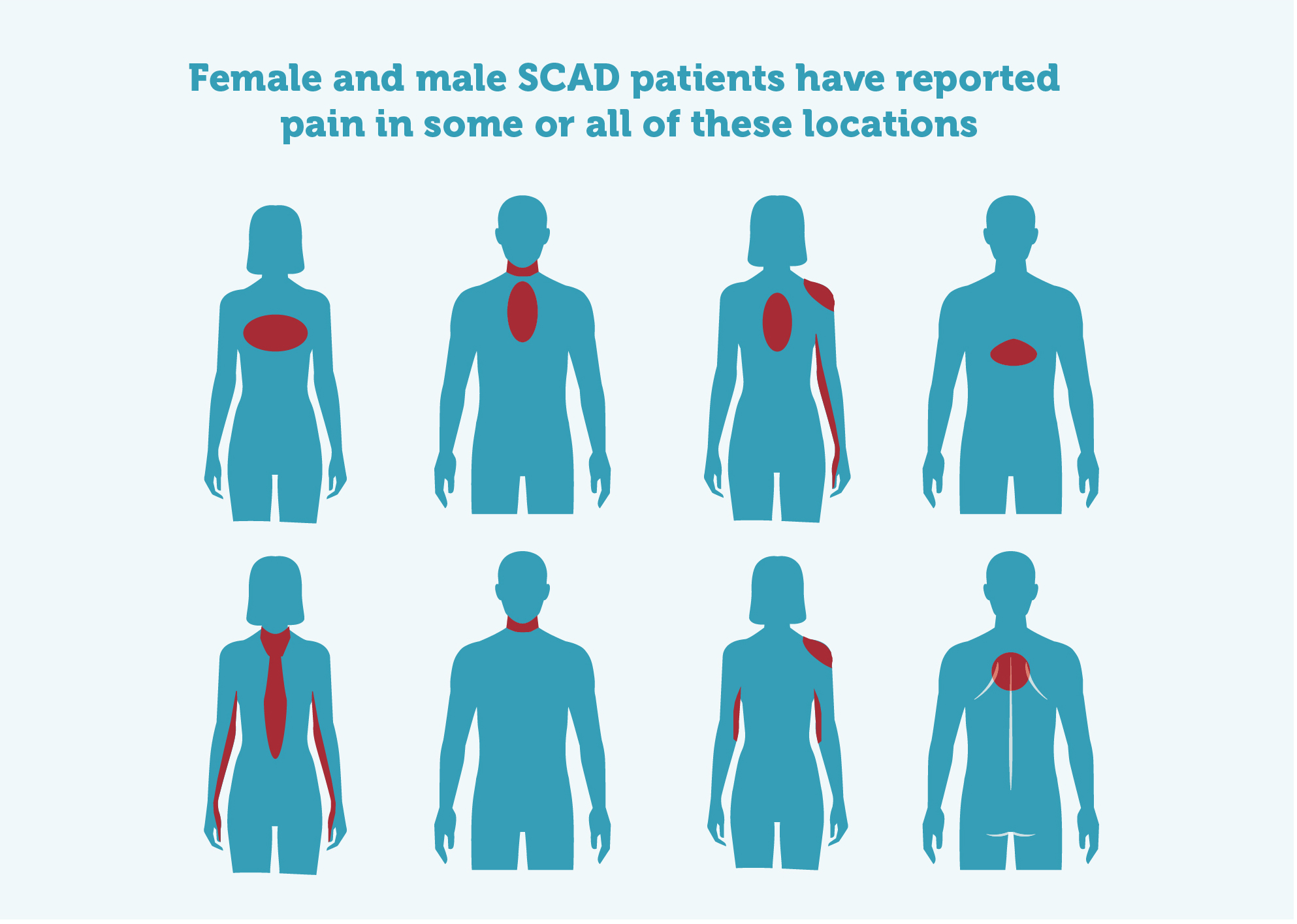
SCAD patients experience different symptoms; the most common are:
- Central chest pain
- Pain or numbness in one or both arms
- Jaw pain
- Back pain
- Shoulder pain
- Nausea
- Sweating/clamminess
- Difficulty breathing
Getting a diagnosis
Chest pain in young, fit people with no history of or risk factors for heart disease, is often dismissed as anxiety, panic attacks, indigestion, gall stones and other conditions.
It’s important that a diagnosis of SCAD is not delayed. The sooner a diagnosis is made, the better the outcome is likely to be. The longer blood flow is reduced, the higher the chance of permanent damage to heart muscle.
Tests to diagnose heart attacks and SCAD include:
- ECG (electrocardiogram) – although ECGs can look normal in some SCAD patients
- Blood tests to assess Troponin levels. (Troponin is a protein that is released into the blood during a heart attack – read more in the FAQ below)
- Angiogram
- CT scan
You may also be given an Echocardiogram which shows how well the heart is functioning and what your Ejection Fraction is (see FAQ below for more).
Current best practice is that patients should be monitored in hospital for at least five days because the majority of recurrent SCADs occur during early follow-up.
See more about diagnosing heart attacks on the NHS website.
Complete the Download form to request our leaflets.
Click on the links below for information about Recurrence, SCAD and Genetics. Patients who would like to request a referral to a SCAD specialist should have a look at the Clinic Referrals page.
Symptoms & Diagnosis…
FAQs
There is a lot of useful and accurate information on the internet about heart disease and heart attacks, however there are also many myths and ‘suggestions’ that are inaccurate and could be harmful if believed or followed.
For example, the ‘cough CPR’ myth that suggests coughing could help if you think you’re having a heart attack or have had a cardiac arrest. There is no medical evidence to suggest that coughing could prevent a heart attack. And CPR is only needed if you have had a cardiac arrest and are unconscious, so you would be unable to cough at that point.
Check trusted sources of information , such as Beat SCAD, the British Heart Foundation , Heart Research UK , Resuscitation Council UK , the NHS or other sites relevant to your query.
You can ask your GP or pharmacy for information too.
Please don’t spread inaccurate and harmful information. If in doubt… check it out!
SCAD patients experience different symptoms; the most common are:
- Central chest pain
- Pain or numbness in one or both arms
- Jaw pain
- Back pain
- Shoulder pain
- Nausea
- Sweating/clamminess
- Difficulty breathing
It’s important that a diagnosis of SCAD is not delayed. The sooner a diagnosis is made, the better the outcome is likely to be. The longer blood flow is reduced, the higher the chance of permanent damage to heart muscles.
Tests to diagnose heart attacks and SCAD include:
- ECG (electrocardiogram) – although ECGs can look normal in some SCAD patients
- Blood tests to assess Troponin levels. (Troponin is a protein that is released into the blood during a heart attack – read more in the FAQ below)
- Angiogram
- CT scan
You may also be given an Echocardiogram which shows how well the heart is functioning and what your Ejection Fraction is (see FAQ below for more).
Current best practice is that patients should be monitored in hospital for at least five days because the majority of recurrent SCADs occur during early follow-up.
There are a number of causes for chest pain. This article from the BHF explains more.
Troponin is a protein that is released into the bloodstream during a heart attack. Raised Troponin blood test results are often part of the process that leads to a SCAD diagnosis. Raised troponin levels, together with other heart attack symptoms, should result in a request for an angiogram to confirm the diagnosis.
Troponin levels in the blood typically increase within 3-12 hours from the beginning of chest pain, peak at 24-48 hours, and return to their baseline over 5-14 days.
Measurement of Troponin levels for patients with chest pain in A&E has been studied widely. Baseline measurement of troponin levels, followed by serial measurements of troponin three hours afterwards, should be performed. Both the absolute value of the troponin level as well as the degree of change in the troponin level should be considered.
It is now understood that women may experience a heart attack at a lower level of Troponin in the blood than men. A higher sensitivity Troponin blood test has been developed and is currently being tested. Currently this is not available at every A&E.
We asked SCAD expert Dr David Adlam if SCAD always causes a heart attack? He told us: It depends on definitions – the overwhelming majority of SCAD patients will present with an acute event (sudden onset) and there will be a rise in the cardiac enzymes which are an indicator of a heart attack. There are some patients who don’t seem to have a rise, but in most cases the patients’ presentation is some time after the event. In this cardiac MRI study, there were 40% of patients where there was no demonstrable injury in terms of a scar. So many of the patients who have the smaller event will not have a persisting heart injury of any size that will be important going forward in terms of the heart function.
Ejection fraction (EF) refers to how well the left ventricle (the heart’s main pumping chamber) pumps blood with each heart beat. Most times, EF refers to the amount of blood being pumped out of the left ventricle each time it contracts.
Your EF is expressed as a percentage.
- 55-70% is considered normal
- 40-54% the pumping ability of your heart is considered slightly below normal, but you may not have any symptoms
- 35-39% the pumping ability of your heart is considered moderately below normal and you may have mild heart failure
- less than 35% the pumping ability of your heart is considered severely below normal and you are likely to have moderate to severe heart failure
SCAD patients should note that Ejection Fraction measurement is not an indication of whether your SCAD has healed or not. EF is often checked during an echocardiogram at the time of the SCAD and then later (6-12 months after the SCAD). Any improvement seen in the overall results of a follow up echocardiogram can be viewed as signs of the SCAD healing process. Ejection Fraction has regularly been seen to improve in SCAD patients over time, particularly after use of appropriate medications and lots of rest to allow the heart to heal.
Click on the links below for more information about Ejection Fraction and Heart Failure.
Migraines happen with increased frequency in SCAD patients. The GWAS (Genome Wide Association Study) on SCAD, published in 2023, identified 16 genetic variants that confer a higher risk of having a SCAD, but it is not caused by a single gene in the same way hereditary diseases are. These genetic variants can be likened to the 'hand of cards' we're dealt at birth (our genetic make-up) – each person will have a different combination of many common variants and it is this combination that can increase the risk of having a SCAD.
One of these variants, PHACTR1, is associated with the risk of migraine and many SCAD patients have reported suffering from migraines. More research is needed to find out more.
Experts say migraine management can be tried using a range of alternative approaches (including topiramate, riboflavin, magnesium, flunarizine, lamotrigine, amitriptyline and valproate). Please check with your GP or cardiologist before starting, stopping or changing any medication.
Find out more by watching these videos:
Beat SCAD Conference 2023 (from about 25 minutes)
Dr David Adlam explains the findings PHACTR1.
Dr Adlam explains the findings of the GWAS paper.