The information on this page is aimed mainly at healthcare professionals caring for a patient with a suspected SCAD. Advice for patients who think they may be having a SCAD is also included.
For detailed information on SCAD see our For Professionals section.
Healthcare Professionals
SCAD can lead to long-term heart damage and can (rarely) be fatal.
It’s important that a SCAD diagnosis is not delayed. The longer blood flow through a coronary artery is reduced or stopped, the higher the chance of permanent damage to heart muscle.
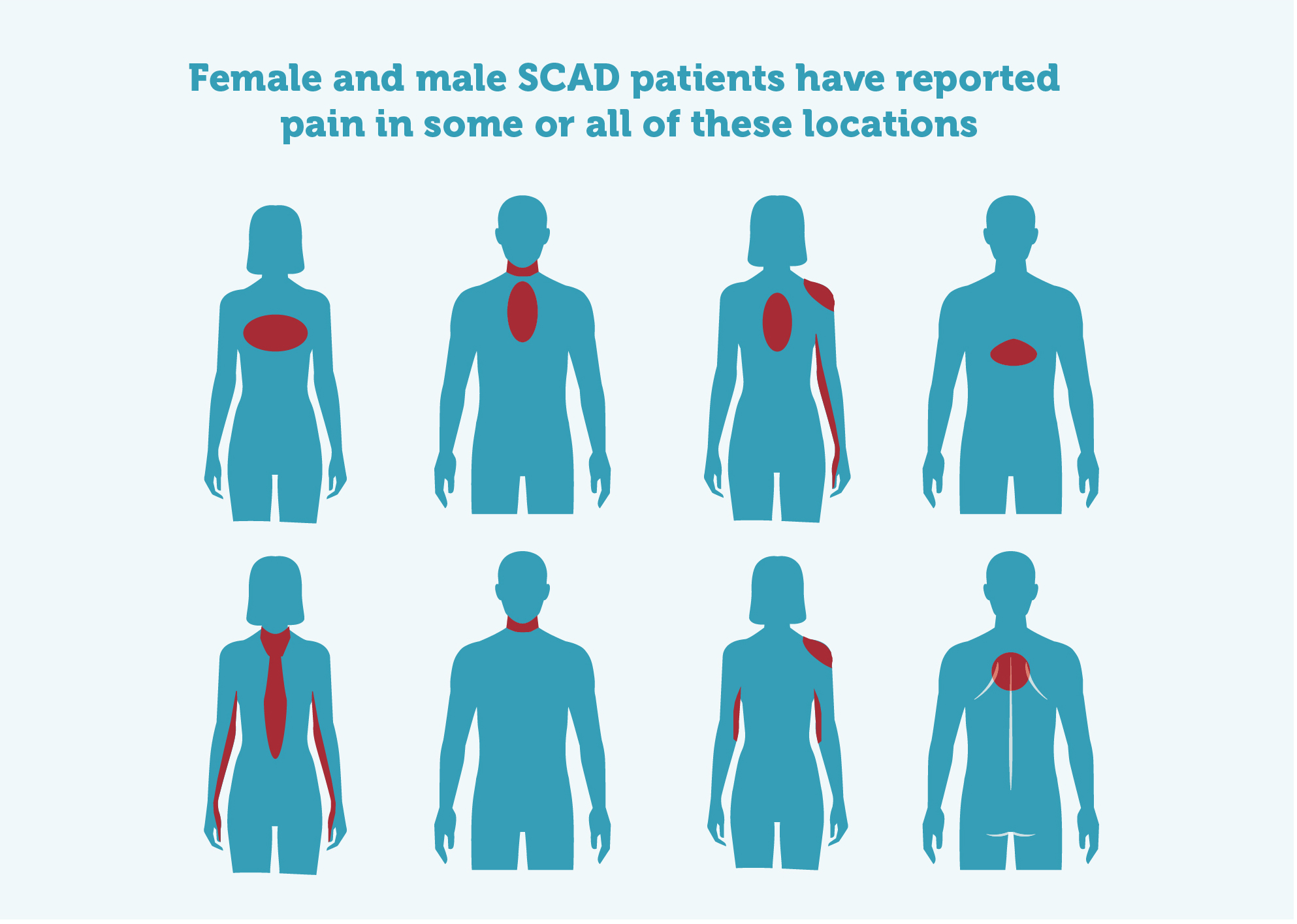
Typical symptoms*:
- Central chest pain
- Pain or numbness in one or both arms
- Jaw pain
- Back pain
- Shoulder pain
- Nausea
- Sweating/clamminess
- Difficulty breathing
- Some will have a sense of ‘impending doom’, others will try to convince themselves that their symptoms are anything but ACS
٭Remember, SCAD patients are often younger, more likely to be female and sometimes may have had a recent pregnancy. Atypical symptom presentations are more common in this patient population so consider a lower threshold for further investigations in hospital.
Please consider the risk of conscious and unconscious bias in your patient profiling. Most SCAD patients have classic Acute Coronary Syndrome (ACS) symptoms but may not look like a traditional ACS patient. Specifically, although they may have some traditional risk factors (eg a history of high blood pressure), SCAD patients will often have a lower risk profile than atherosclerotic heart attack patients.
SCAD facts…
- ~90% female, about 10% male
- Most are young to middle-aged, average age around 50 (but SCAD has been reported in patients aged 18-84)
- All ethnicities may be affected
- Pregnant/post-partum – 10% of cases of SCAD overall but SCAD accounts for 21-27% of heart attacks in pregnancy
- 50% of post-partum coronary events are reportedly due to SCAD
SCAD patient experiences: Treat the symptoms not the profile
Remember to treat the symptoms you see in front of you – not the patient's risk profile – and please check your bias. SCAD patients tell us that because they often have few/no cardiac risk factors:
- They get told they have indigestion or are having a panic attack when they are, in fact, mid heart-attack.
- Male SCAD patients are often treated like patients with atherosclerosis.
- Many patients get asked if they have recently used cocaine…
- Pregnant or post-partum patients are told they’re ‘too full of hormones’ to be having a heart attack.
Paramedics – actions in the case of suspected SCAD:
- Undertake ECG (may be normal)
- Triage to a cardiac centre and transport with pre-alert
- Advocate for patient on handover and reinforce the need for troponin testing*
* remembering receiving teams may be unfamiliar with SCAD and elevated troponin may be the only early diagnostic indicator
A&E Staff – check Troponin levels
- Perform promptly and then repeat a Troponin blood test according to local protocols for ACS. Explain that it is best to stay in hospital until the results are back.
Cardiology Staff – take care when performing angiograms
- Check Troponin results
- Angiograms (see the chapter on SCAD in The PCR-EAPCI Textbook)
- necessary to confirm diagnosis but consider stability of patient before performing
- gentle catheter technique essential
- low threshold for OCT imaging where diagnostic uncertainty remains after initial angiography
- conservative management optimal if patient is stable
- if stenting required, expect more complications than for patients with atherosclerosis
- avoid repeat angiograms unless patient is unstable (and never to ‘check for healing’)
- CT coronary angiography (CTCA) has a high false negative rate in SCAD patients. Normal CTCA does not exclude SCAD
- not sure of the diagnosis or best management? Diagnosis can sometimes be difficult. Clinicians, please contact the Leicester SCAD service (Dr Adlam) directly 24/7 via Glenfield Hospital switchboard or the SCAD email scad@uhl-tr.nhs.uk
- In-hospital monitoring
- Where conservative management fails, the majority of recurrent SCAD cases occur during early follow-up, so monitoring in hospital for at least five days is advised in conservatively managed SCAD patients.
SCAD Patients
If you have had a SCAD and think you are having another one or suspect you or someone you are with is having a SCAD, don’t ignore cardiac symptoms.
- Don’t delay: time = heart muscle
- Check: Symptoms of a heart attack on the NHS website
- Dial 999: state “suspected heart attack”, describe symptoms
- Time to go: get the patient to a cardiac centre
- Troponin blood test required (see FAQ on Symptoms and Diagnosis page for more information about Troponin tests)
- Share our SCAD for health professionals leaflet and this page with any healthcare professional you talk to